Modified from an article published in the AMA (WA) journal Medicus, March 2015
By Dr Stephanie Davies
Director, WA Specialist Pain Services (WASPS)
 Pain can be, and often is, complex to understand, so it is not surprising that it can be a challenge to treat. Pain is a subjective experience and objective measures of its presence and consequences are not achieved by modalities usually used by medicine such as blood assays and imaging. Alternative measures which explore the psychosocial effects of chronic pain need to be used. Chronic pain is not amenable to the paradigms of biomedical treatment which promote passive management; in particular there are significant limitations to the role of analgesics. These issues are explored in this article and an effective management approach, pioneered in Western Australia, is described.
Pain can be, and often is, complex to understand, so it is not surprising that it can be a challenge to treat. Pain is a subjective experience and objective measures of its presence and consequences are not achieved by modalities usually used by medicine such as blood assays and imaging. Alternative measures which explore the psychosocial effects of chronic pain need to be used. Chronic pain is not amenable to the paradigms of biomedical treatment which promote passive management; in particular there are significant limitations to the role of analgesics. These issues are explored in this article and an effective management approach, pioneered in Western Australia, is described.
For most people with pain there aren’t any current biochemical markers for pain that show up on blood tests.
Pain is invisible on routinely available radiological imaging. Hence, the disconnect between pathology routinely reported on radiological imaging and the presence or absence of concordant pain[1]. Changes seen in spinal x-rays are age-related and often unaccompanied by pain. By contrast, spinal pain can be present in the absence of such changes. It is important to remember that imaging does not show pain – imaging shows anatomy[2]. Magnetic resonance imaging (MRI) can provide additional information, for example, high intensity zones associated with discogenic pain[3], chemical radiculitis and fat infiltration of lumbar multifidi muscles associated with lumbar back pain in adults[4] (not adolescents), however these findings are not always reported. Functional MRI’s, including spinal cord imaging[5], might provide more information on the motor and sensory networks in the future.
Studies at a microscopic level do demonstrate changes in the nervous system – for example in immune-responsive glia, in neurotransmitters and in receptors[6]. These changes within the nerves, spinal cord and brain are known to occur, but are hard to quantify whilst the patients are alive – notwithstanding fascinating studies using functional MRIs which show differences in blood flow to regions of the brain when pain is studied across a range of changeable factors including mindfulness, virtual reality, and empathy.
Major advances have occurred in understanding how glia and immune cells in the nervous system respond to painful inputs and contribute to persistent pain. Some very clever researchers are showing that immune-like cells in the brain, spinal cord and peripheral nerves play a major role in all forms of pain. In the central nervous system there is an immune-like response when an organism is under danger or threat: microglia and astrocytes become activated. Examples of such threats are infection and psychosocial stresses. The glia detect and remember “threats”; if significant nociception (hyper-nociception) occurs, the response is transformed by the “glial memory”. Thus these two components – glial activation and hyper-nociception — rewire the nervous system to maintain persistent pain[7].
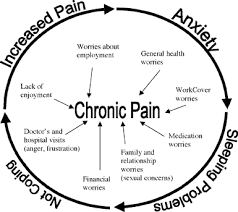 Anger, stress and distress increase the “threat” value of pain and therefore they increase the likelihood of persistent pain and disability. The implication of this is that feelings of stress, worry and being under threat need to be removed. This is a key point, because pain intrinsically makes make people feel anxious or worried: this results in pain being an effective alarm signal so that survival of the organism increases by avoiding the threat. However, if a potential threat is more perceived rather than an actual threat, then the resultant persistent pain is amplified without benefit to the organism surviving. That is, we are all wired as a biological imperative to respond to and avoid pain and injury, but unhelpful amplification of “threat” results in unhelpful “alloplastic” pain. One of the major roles an effective health professional can play is to reduce the threat value of pain. Therefore it is critical to use tools which assess the patient’s psychosocial situation, including their beliefs about their pain and disability.
Anger, stress and distress increase the “threat” value of pain and therefore they increase the likelihood of persistent pain and disability. The implication of this is that feelings of stress, worry and being under threat need to be removed. This is a key point, because pain intrinsically makes make people feel anxious or worried: this results in pain being an effective alarm signal so that survival of the organism increases by avoiding the threat. However, if a potential threat is more perceived rather than an actual threat, then the resultant persistent pain is amplified without benefit to the organism surviving. That is, we are all wired as a biological imperative to respond to and avoid pain and injury, but unhelpful amplification of “threat” results in unhelpful “alloplastic” pain. One of the major roles an effective health professional can play is to reduce the threat value of pain. Therefore it is critical to use tools which assess the patient’s psychosocial situation, including their beliefs about their pain and disability.
Alloplastic pain means the ‘other’, ‘changeable’ pain and reflects complex, interactive and systemic (holistic) processes, occurring in-and-around the organism in pain. Such processes are likely to be active at a cellular, genetic,neurological (including psycho-cognitive & autonomic), immunological, endocrine and environmental level which together may be seen as systemic core-pain responses. See: What is Pain? E.Visser, S.Davies. Australian Anaesthesia 2009
In WA, it has been uncommon to see assessments that include validated questionnaires that measure the injured worker’s biopsychosocial risk of disability such as the Orebro musculoskeletal questionnaire (OMPQ for persistent pain) or StartBack (low back pain). Further, it is not routine practice, outside of pain medicine, to use screening questionnaires for neuropathic pain (such as Pain Detect); nor pain and function (such as Brief Pain Inventory, Pain Disability, Roland Morris or Oswestry); whilst the use of instruments that are validated for people with persistent pain to measure anxiety and depression such as HADS and the DASS are not seen outside multidisciplinary pain services – yet anxiety is enmeshed in the experience of pain.
The biopsychosocial model of assessment and management of people with pain isn’t new. It has been part of the teaching of pain medicine to doctors and health care professionals since I was a registrar in the mid 1990’s.
What is new is that in the last decade a range of healthcare professionals and managers have worked extremely hard to provide systems that easily provide both pain education and skills to be taught as the ‘first-line’ treatment to people with complex persistent pain.
In 2007, Fremantle Hospital & Health Service Pain Medicine Unit introduced the Self-Training Educative Pain Sessions (STEPS), an eight hour pre-program held over two days, which 70-80% of people attend prior to individual consultations. This was funded via a translational research grant in 2007-2008 from SHRAC (WA DOH).
The STEPS pre-program, i.e. before entry to the clinic, taught pain knowledge including neuroplasticity, and skills such as pacing, pain approach, mindfulness, making sense of pain, and medical options. The key healthcare professionals were pain physicians, musculoskeletal physiotherapists, behavioural psychologists and occupational therapists. In this tertiary sector, from 2007 to 2014 approximately 3000 patients attended the Fremantle Hospital STEPS program, halving the unit cost of a referred new patient as well as dramatically reducing waiting time as the capacity of the unit to see new patients increased (doubled) because patients were able to more readily engage and implement with non-medically focused options. Sir Charles Gairdner Hospital and Royal Perth Hospital have similar pre-entry group programs.
The focus is shifted to what the patient can do, such as pacing activities, paced daily walk, non-vigorous movements, pain approach, mindfulness, relaxation, acceptance, and reduction of life stressors. This last point is vital as many people are juggling several or many life stressors.
One of the skills we teach patients is to reduce the time spent thinking on issues that can’t be worked on, or solved, any time soon. Each minute spent running through the problems (in their head) makes them feel bad and pushes mood down. Patients are encouraged to try using the ‘3 D’s approach’ – “Do it, Delegate it, or Dump it” (I use this as my mantra): “do it” can be implemented by devising realistic achievable goals; “dump it” can be implemented by avoiding unhelpful emotions when negative events occur, using the analogy of the “dead bat” [definition as per http://www.wikpedia.com.]
Verb – dead bat (transitive, cricket): To play (the ball) with a dead bat.
Noun – dead bat (cricket): The bat when held with a light grip such that it gives when the ball strikes it, and the ball loses momentum and falls to the ground.
Our tracking of the Fremantle Hospital participants who returned validated questionnaires from October 2007 to the end of 2009 showed that the hundreds of participants had implemented an increased number of active pain strategies and had improved abilities to do daily chores, i.e. they had less disability.
The expansion of co-ordinated pain services to Medicare Locals, STEPS-PNML, STEPS-BAML and STEPS-PSCML, started ![]() in 2011: to date about 300 patients have attended these group programs. Its intent was to bridge the gap in primary to secondary care for people with persistent pain who had a less complex mix of co-morbidities. It comprises attendance at the two day STEPS program combined with a one-off pain team assessment (physiotherapist, behavioural psychologist, pain physician) to provide support to the patient (and significant others) as well as community healthcare professionals.
in 2011: to date about 300 patients have attended these group programs. Its intent was to bridge the gap in primary to secondary care for people with persistent pain who had a less complex mix of co-morbidities. It comprises attendance at the two day STEPS program combined with a one-off pain team assessment (physiotherapist, behavioural psychologist, pain physician) to provide support to the patient (and significant others) as well as community healthcare professionals.
Subsequent care is filtered to either primary care (less complex) or tertiary care (more complex) depending on the management plan made by the pain team. These programs help people with pain to improve function and return to a more normal life. The positive feedback from patients and their families recognising that they feel empowered, with more control, is significant, as well as improving health outcomes for these participants and leading to significantly reduced waiting times at the tertiary pain clinics in WA.
Patients with a high number of complex issues continue to require access to existing tertiary services to access the expertise and experience of specialised healthcare professionals, investigations, interventional pain procedures, non-PBS medications, and to receive the ongoing care that is required for people in pain with multiple medical co-morbidities, co-existing mental health conditions, and complex medication regimes (including S8 opioids); also they may need to attend more intense (longer) cognitive behavioural group programs.
Future analysis of the triage information will enable – hopefully – a simple tool for assisting services in determining the optimal referral pathway between primary-secondary and tertiary services.
The emphasis here is that pain is often complex and requires a multi-modal approach to address the multidimensional nature of pain. An engaging patient-centred approach drawing upon the expertise of multiple healthcare disciplines is emerging as the best practice to tackle pain (as well as other chronic conditions).
I feel it will take clinical leaders working with health managers and politicians to produce sustainable systems to allow growth in the future for people in pain and people with other complex conditions. The current challenge is how to move forward in a health-economic responsible manner.

Dr Stephanie Davies is also Adj. A/Prof, Curtin University, School of Physiotherapy; Senior Lecturer, UWA, School of Medicine and Pharmacology; Chair State Wide Pain Services (SWPS); Co-Chair Pain Health Working Group (PHWG); and Director of Cocare.io and WA Specialist Pain Services (WASPS).
The author gratefully acknowledges the extensive consultation with Dr Will Howard when revising this article for publication.
[1] Rubinstein SM, van Tulder M. A best-evidence review of diagnostic procedures for neck and low-back pain. Best Pract Res Clin Rheumatol. 2008;22:471–482.
[2] Yelland M1 Diagnostic imaging for back pain. Aust Fam Physician. 2004 Jun;33(6):415-9.
[3] Aprill C1, Bogduk N, High-intensity zone: a diagnostic sign of painful lumbar disc on magnetic resonance imaging. Br J Radiol. 1992 May;65(773):361-9.
[4] Kjaer P1, Bendix T, Sorensen JS, Korsholm L, Leboeuf-Yde CAre MRI-defined fat infiltrations in the multifidus muscles associated with low back pain? BMC Med. 2007 Jan 25;5:2.
[5] Eippert and Tracey. The spinal cord is never at rest. eLife 2014;3:e03811. DOI: 10.7554/eLife.03811
[6] Kaufmann I1, Eisner C, Richter P, Huge V, Beyer A, Chouker A, Schelling G, Thiel M. Psychoneuroendocrine stress response may impair neutrophil function in complex regional pain syndrome; Clin Immunol. 2007 Oct;125(1):103-11. Epub 2007 Aug 16.
[7] Grace PM, Hutchinson MR, Maier SF, Watkins LR. Pathological pain and the neuroimmune interface. Nat Rev Immunol. 2014 Apr;14(4):217-31







Hi John,
The current information as per the Grace et al updates the view on synapses.
Always good to hear others viewpoints.
Cheers
Steph
Steph, the theme of the outstanding review performed by Grace et al. is that of dysregulation of central neuro-immune signaling mechanisms. I could not find any mention of “unhelpful amplification of threat”. However, they do mention the possibility that microglia might have a role in coordinating diverse responses to insult. It would be helpful to me if you outlined those operational criteria for “alloplastic pain” that would enable it to be distinguished from nociceptive and neuropathic pain states.
Stephanie, I enjoyed reading your article. But from my understanding, the experience that we call “pain,” like all other of our experiences, is changeable. Therefore, according to your definition, the experience of pain must be “alloplastic”. But you go on to assert that “unhelpful amplification of threat results in unhelpful “alloplastic” pain.” I am not sure exactly what you mean by this. Can you please explain?
Hi John,
“we are all wired as a biological imperative to respond to and avoid pain and injury, but unhelpful amplification of “threat” results in unhelpful “alloplastic” pain”.
This links back to the immune-like cells in the central nervous system (the reference to the Grace et al article). Glia get triggered when the is both threat and hyper-nociception, and end result of this is a tetrapartite or pentapartite junction with the neuronal synapses.
This is relevant if the perceived threat is greater than the likely threat to the organism. It is this “unhelpful” component that I am referring to in both the amplification of threat and also the alloplastic pain.
Cheers
Steph
Thanks Steph. Neuronal synapses can only “know” about other neuronal synapses. It is the whole organism (i.e. person, in this case) that determines the salience of a perceived existential threat relative to its current state. I don’t think “alloplastic” cuts the mustard in this context.