A brief report on preliminary results by Professor Michael Nicholas
The study was led by Michael Nicholas, Director of Pain Education and Pain Management Programs at the Pain Management Research Institute (PMRI), in collaboration with and colleagues at NSW Department of Health, iCare (Insurance & Care NSW) and Employers Mutual Workers Compensation (EML). Recently, EML won the Swiss RE Excellence & Innovation in Return to Work Award 2015/2016, highlighting the importance of early intervention to improve return to work rates after injury.
The interim results from this 2.5 years study were presented in November (2015) at the TMF-iCare conference in Sydney (TMF is Treasury Managed Funds, which provides the financial underpinning of all public sector workers compensation funding in NSW; icare is the new umbrella organisation for all compensation insurance in NSW). The final results will be available later this year, but so far they seem consistent with what is presented here.
Briefly, the study involves identifying (within a week of injury) injured workers who may be at risk of delayed recovery/return to work (RTW) and treating them according to a protocol supported by the key stakeholders (workplace, insurer, treatment providers, and insurance scheme regulator). Critically, this is a multi-level intervention, with no particular treatment specified. In fact, the same treatments were available to both Intervention and Control groups. It was funded by a consortium comprising the NSW Ministry of Health (MoH), icare (TMF), and EML Workers Compensation insurance, and we (PMRI/Kolling/University of Sydney) provided the research expertise.
We wanted to test out a protocol for the early management of injured health workers (with soft tissue injuries) to test whether they could be returned to work sooner and more sustainably than what was being achieved by usual care and at less overall cost. An earlier pilot trial at Concord Hospital in the mid 2000’s (and presented at the Adelaide APS meeting in 2009) showed the concept was feasible, but a larger controlled trial involving multiple hospitals was required to confirm the results.
At risk injured workers were identified by a brief screening questionnaire (for psychological risk factors – the OMPSQ-short form developed by Steven Linton and colleagues in Sweden1). This was administered to consenting workers (who had taken a medically-approved week off work) by the insurance case manager by phone within 7 days of the injury. 580 Injured health workers from 17 hospitals in the Sydney region and further south/west (all covered by one insurer, EML) were used in the study. The hospitals were divided into Intervention and Control conditions for the duration of the study.
The high risk cases from the Control hospitals were managed according to current NSW WorkCover guidelines for soft tissue injuries. In the Intervention group the high risk injured workers also had whatever treatment their GPs thought appropriate plus access to a psychologist (within 2-3 weeks of the injury) to address identified psychosocial obstacles for RTW. The participating psychologists agreed to follow the protocol and to liaise with the workplace and treating doctor at least once a fortnight on progress with each case. The psychologists were free to employ whatever treatment they thought appropriate to the case (within 6 sessions). The injured workers in the Intervention group were also reviewed by an independent Occupational Physician (or similar) within 6-8 weeks to reassure them (and the GPs) they had a soft tissue injury and should recover quickly. A specialist physiotherapist reviewed (from case notes) any physiotherapy requests for more than one plan of 8 sessions. The Intervention workplace was also actively involved in assisting RTW via the RTW coordinator. The management at all participating Intervention hospitals and EML fully supported the process.
The recruitment finished in June 2015 and we have almost completed the 1 year follow-up data collection. Nevertheless, with most data in the results are fairly clear. This is reflected in the MoH’s decision to implement the study protocol across all public hospitals in NSW. This has started for EML-covered hospitals already (Sydney to the VIC border) and all QBE-covered hospitals (Sydney to QLD border) began the process in Feb 2016. Planning work with TMF-icare is also under way to examine extending the implementation across the whole public sector in NSW over the next year.
The results to date show that RTW is greatly enhanced in the Intervention hospitals (Mean lost days for Control hospitals was 53 vs 29 for the Intervention hospitals). Overall, 24% of injured workers screened (of 580) were identified as high risk, and average costs at 6 months were 22% less for the Intervention group over the Controls (about $4,000 per worker, so far). The insurer expects this to rise as the Control group’s costs are continuing to rise, while the Intervention group has reached a plateau (see figures below). The average number of sessions with the psychologists was 5 (at an average cost of about $1,000).
The two figures below depict the lost work time and cumulative cost outcomes. These clearly indicate major benefits for the protocol, and the plateau effect shows these are sustained.
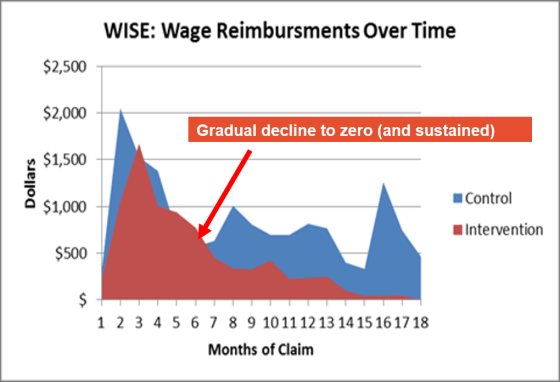
Average Wage Reimbursements over 18 months (=lost time) Key Outcome: Intervention group has less time off work, and it is sustained
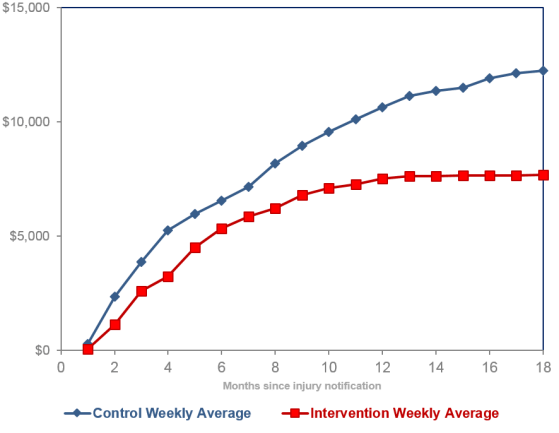
Cumulative average weekly benefits costs Intervention workplace costs plateau; Control (usual practice) is rising
One of the key outcomes we are interested in is whether there is any difference between the groups in the development of chronic pain, but we won’t know this until we can get our hands on the follow-up data. On the basis of our findings we are recommending to the workers compensation regulators and insurers in NSW that the risk screening should be employed for all injured workers who take time off for their injuries and the management protocol should be applied to those who are deemed at high risk. In addition, we argue that any worker who is still off work after 3 months and reports pain is a factor should be referred for a multidisciplinary pain assessment (while they still have a job to return to).
Reference
- Linton SL, Nicholas MK, MacDonald S. Development of a Short Form of the Örebro Musculoskeletal Pain Screening Questionnaire. Spine 2012; 36(22): 1891-95.






